Dirty Sex
Why COVID-19 Hasn’t Been the New ‘Gay Pneumonia’

SARS-CoV-2, the virus that causes COVID-19, left the bowels of a bat in Wuhan, China, and has become the collective pain in the ass for much of the globe’s seven billion residents. It has already infected over 12 million people worldwide and killed over 500,000 in the span of six months. To say it packs a punch is an understatement, since so few diseases rise to these levels or so quickly. In fact, the official term to describe it is “pandemic,” which is an epidemic that has gone worldwide. Whereas your run of the mill outbreak gets a few likes, COVID-19 has gone viral. But unlike a social media post that is clickbait fodder, few people want to experience COVID-19’s less than popular appeal, or do they?
The United States leads the world in both infections and deaths of COVID-19, representing a quarter of cases and of people dead globally. The virus’ singular hold on the U.S. has seen a near halt in economic productivity, unemployment approximating levels unseen since the Great Depression, and has opened nearly every social wound, pitting many Americans against one another.
While the Trump administration’s coronavirus task force, along with the Centers for Disease Control and Prevention (CDC), have prepared guidelines to help states manage their responses to the pandemic, some governors feel the White House hasn’t done enough. The administration’s task force, led by Vice President Mike Pence, who himself was blamed for delaying vital public health measures that resulted in a worsening of an HIV outbreak in 2014 when he was governor of Indiana, has been accused of being too late to respond to the pandemic. Critics, like the state department’s former inspector general who was fired from his post, contended that the administration’s negligence left the country’s medical professionals with inadequate personal protective equipment and testing supplies, and local governments ill-prepared to carry out vital contact tracing that could significantly curb the disease’s spread.
The president has maintained that his administration’s handling of the epidemic has been “perfect” and said publicly in a press briefing in March that he took no responsibility for the country’s lack of preparation. Pundits have argued that by abdicating administrative authority to the governors, the administration hopes to wash its hands of accountability in an election year. States that reopened their economies too early or had never closed them are now in the throes of infection spikes and pondering whether to close down their economies again or whether to reopen schools in the fall. This, all as China and Europe, which had seen similar rates of infection earlier, have drastically reduced the disease in less time and have reported a fraction of the new cases seen in the U.S. Clearly, there hasn’t been a unified strategy in America and the lack of leadership from the White House has been unproductive. It has not only set back economic recovery but has also influenced how people perceive the lethality of the illness. One would think this is the first time the U.S. has had to deal with a national health crisis.
But COVID-19 is not the U.S.’s first bout with a bad bug. June 5, 1981 marked the first published report of an unknown illness affecting gay men, dubbed early on as the “gay pneumonia.” Much like SARS-CoV-2, the human immunodeficiency virus (HIV), is believed to have been transmitted from animals to humans and emerged in the American west. Additionally, the initial symptoms of both diseases presented as largely respiratory-related. Both diseases first infected America’s white population, then nestled themselves in the bodies of Black and brown people disproportionately. But this is where the diseases’ similarities end.
Within the first six months, AIDS had claimed only 337 lives in the U.S., next to COVID-19’s 135,000 and counting in less than four. Whereas it took about a year for any congressional assembly to discuss AIDS, it took a few months for the U.S. to set up congressional meetings to mobilize vaccine research and to handle the economic fallout of COVID-19. It would take another year for the government to assemble a federal response and for congress to approve funds for HIV research in July of 1983. The World Health Organization (WHO) wouldn’t start assessing and monitoring HIV for another four months. This was November of 1983—two and a half years after the first reported HIV case. For SARS-CoV-2 it took one day.
One can suggest that many lessons from the 80s were learned or that hindsight is 20/20 to account for comparative quicker response time by the Trump administration, Congress and the WHO. Indeed, the nation’s experts whom Trump recruited, doctors Deborah Birx and Anthony Fauci, were also heavily involved in the 1980s AIDS crisis. In the case of HIV, much like SARS-CoV-2, the lag could be explained by a lack of experience with a novel virus. But some members of Congress like the former Rep. Henry Waxman, as well as the recently deceased playwright and activist, Larry Kramer, and other activist groups like ACT UP were at the time making a lot of noise for the Reagan administration to take the disease more seriously. To get a sense of the political climate as it relates to gay people, Bill Dannemeyer, the Republican congressman of California, delivered a speech in Congress titled “What Homosexuals Do,” listing graphic details of gay sex and was in favor of legislation to create an AIDS registry, to quarantine patients and to carry out deportations of infected immigrants. At the time, it was also a felony in various states to be gay.
The New York Times didn’t publish its first front page story on the crisis until May of 1983, saying “Health Chief Calls AIDS Battle ‘No. 1 Priority’,” meanwhile 1,450 cases had already been reported and 558 people had died. In the Times article, said health chief, Dr. Edward N. Brandt stated, “We have seen no evidence that it is breaking out from the originally defined high-risk groups,” which at this time were identified as the 4-H club of homosexuals, hemophiliacs, heroin addicts and Haitians. Brandt ended with, “I personally do not think there is any reason for panic among the general population.” This admission didn’t quell the hysteria of the public who wondered whether they could get infected through casual contact.
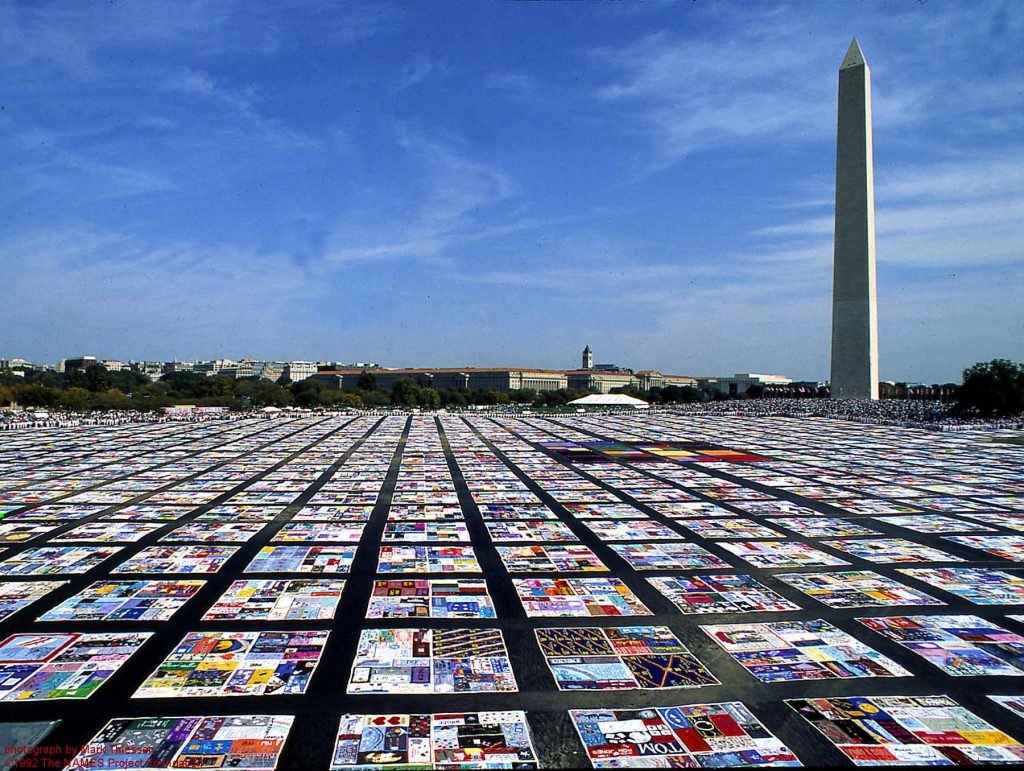
It wasn’t until AIDS was found in children and heterosexuals that were neither drug addled nor had gotten transfusions that the “gay pneumonia” was taken seriously, officially named and considered an epidemic. By then it was too late and the lackluster response from government officials was voluminous to the community it was mostly afflicting. Six years in, an infamous quilt made up of 1,290 three by six feet panels (the standard dimension of a grave) draped the lawn of the Washington Monument to memorialize the 20,000 people whose deaths it seemed the government had seemingly ignored and whose deaths many families wouldn’t recognize because of the sexuality of their sons or the association with the disease. That same year, President Regan formed a commission to investigate the pandemic. The number of Americans who have died from AIDS is now over 700,000 and HIV has become the bogeyman of diseases, even as it’s been tamed into a more manageable, chronic condition with therapeutics or made undetectable.
Why are so many Americans willing to go it bareback in the absence of a vaccine?
Recall that a pandemic is an epidemic that has gone global. In the above context, with COVID-19 having a higher infection and case fatality rate than the AIDS epidemic in its early days, it seems the governmental response and especially the public concern for COVID-19 is not proportionate to its severity. In other words, there shouldn’t have been any equivocating, knowing what we know about HIV that was harder to contract but which ultimately proved devastating, especially when we are faced with a larger crisis that has no cure and won’t for more than a year. Instead, it became polarized because of the president and Republican governors who have pitted their constituents against scientific recommendations considered too aggressive, a threat to their civil liberties, and bad for Trump’s economy.
By decrying the very practices that would shorten the lifespan of the pandemic, they instead lengthened it. Such is the case that the idea of wearing a mask, SARS-CoV-2’s equivalent of a condom, and which has been proven to lower infection rates, has become politicized with many in largely red states unwilling to wear it. (The governor of Texas has since reversed course and has made it mandatory.) Instead of articulating the true seriousness of the disease, the Trump administration has chosen to minimize it. At the Rally in Tulsa, Oklahoma, Trump said to an approving crowd of supporters the majority of whom were not wearing masks or social distancing, “When you do testing to that extent, you’re going to find more people, you’re going to find more cases. So, I told my people slow the testing down, please,” which he reaffirmed the following day, because he felt the increasing numbers make him look bad rather than serving the interest of the public to understand the prevalence of the virus. It asks the question: why is there this dissonance and why are so many Americans willing to go it bareback in the absence of a vaccine?
The easy answer is that the large majority of people infected with SARS-CoV-2 recover from the disease and it is a disease that affects everyone, although it mostly impacts the elderly, and Black and brown populations disproportionately. Remember that COVID-19 is more infectious and lethal than HIV was in its first few months before there were therapeutic drugs. While comparing today’s numbers for both ailments would be misleading, as AIDS kills at a slower pace than COVID-19 and is ameliorated by effective drugs, COVID-19, on the other hand, kills in days or weeks and has no current vaccine. Often characterized as a disease affecting the elderly, SARS-CoV-2 has killed many younger than 50. Broadway actor, Nick Cordero (41), being a recent and famous victim. The states seeing the highest spikes, like Florida, Texas and Arizona, currently report the average age of infection is younger than 40. In fact, some 7.5% of US COVID-19 deaths are of people 54 years old or younger. Combined, there are fewer than 2 million cases in the U.S. of HIV, including those who have died of the disease in its 40 year history vs over 3 million positive cases and death attributed to SARS-CoV-2 in less than four months. While the majority of those stricken with the SARS-CoV-2 recover, stats from the UK suggest that 50% of those who got hospitalized in that sovereign nation still reported respiratory, cardiac and neurological ailments months later and were in need of moderate to acute care. Playing Russian Roulette with the disease means that some portion of the time COVID’s barrel will not come up empty. There is much still unknown about any potential lingering effects from the novel virus or what level of immunity one has from being infected with it, or even what happens to the body if you catch it again when your immunity wears off. So, the true answer why many Americans are cavalier about COVID-19 is therefore far more complex.
Many critics in the media point to the Trump administration’s mischaracterization of the disease, which the administration first described as being similar to the flu and which Trump said would “wash through” in a month and later questioned if it could be remedied by injections with disinfectants like bleach and Lysol. Some, including the White House, fault the WHO and the Chinese government for not disclosing the severity of the situation in late 2019. Some blame the CDC for its evolving warnings and policies, like wearing a mask. Still others accuse the media for focusing more on the administration’s misinformation than in uncovering the facts and properly educating the public. The truth is it’s a mixture of all the above.
Since the Trump administration is the single authority setting the agenda for the states to execute and the administration chose to communicate with the public about the disease in daily press briefings, they can’t absolve themselves of much of the responsibility. Especially where, in some cases, they shortcut or flout scientific recommendations, including from members of the White House’s own coronavirus task force like the nation’s leading infectious disease expert, Dr. Fauci. It’s been reported that Fauci has not briefed the president in the last two months and that the White House has been actively marginalizing Fauci, which the White House denies, because of his warnings that run in contrast to the administration’s characterization of the handling of the pandemic. Described as a discrediting campaign, a White House official provided a list to NBC News and The Washington Post of some dozen statements officials say illustrate that Fauci has been wrong about the disease over the last few months. The list is reported to include comments on the level of risk for a U.S. outbreak earlier in the year, recommendations on whether to halt travel between China and the U.S., and whether wearing a mask was necessary. It wasn’t so much that Fauci’s comments were erroneous as they were based on what was known about the disease at the time.
Four former directors of the CDC who have served under Democratic and Republican presidents have since come out, rebuking the administration for undermining science and its own CDC guidelines, saying in a Washington Post article, “Sound science is being challenged with partisan potshots, sowing confusion and mistrust at a time when the American people need leadership, expertise and clarity. Public servants have been harassed, threatened and forced to resign when we need them most. This is unconscionable and dangerous.”
When Freshfruit asked the WHO about what the U.S. is doing wrong, the WHO said in a statement, “Countries can reduce both the transmissibility and severity of the virus by putting in place public health measures in a whole-of-society approach. No testing alone, no physical distancing alone, no contact tracing alone, no masks alone; do it all. Countries that have adapted this comprehensive approach have suppressed transmission and saved lives.”
As was learned in the 80s, how a President handles a crisis helps to shape public opinion and can directly impact the number of lives lost, as the bearer of the loudest megaphone. In the case of Reagan who didn’t utter the words AIDS publicly until 1985, it bolstered the idea that HIV was a gay disease not for public concern and perhaps one gay men deserved. At the time there was tremendous anti-gay fervor to halt the gay rights movement by evangelical Christians as well as the openly anti-gay senator Jesse Helms, who helped to pass law to block the Federal Centers for Disease Control from funding AIDS programs. Had the Reagan administration acted sooner, it could have minimized the spread of the disease by accelerating research, educating the public to contain the disease faster and minimize loss of life.
In Trump’s case, his desire to frame the disease as of minimal concern, even being unwilling to wear a mask publicly until last week, made wearing a mask political and the disease seem trivial. His behavior has led to a lot of misinformation and misguidance that could be responsible for needless deaths or injury. There’s a twisted irony in Trump’s action because being over 70 years old puts the president among the population with the highest risk. And yet, Trump has ramped up daily testing for those in his immediate surroundings so that they don’t infect him — a courtesy he doesn’t extend to those who attend his rallies and who must waive their right to sue him should they contract the virus at his events. So far, six members of the president’s Secret Service staff tested positive before the Tulsa rally and two afterwards. One of the president’s valet’s, the vice president’s press secretary, and Kimberly Guilfoyle, Donald Trump Jr.’s girlfriend, also tested positive. Trump might have learned a lesson from similar hubris of fellow right-wing populist, Jair Bolsonaro of Brazil, and the U.K.’s Boris Johnson — both science deniers, COVID-19 survivors and the latter a reclaimed mask proponent.
How many people deemed as having the lowest risk would willingly stand before a loaded shotgun, knowing that 7.5% of the time they will get a direct and fatal hit?
Just like HIV was minimized and stigmatized as an illness affecting gay men, SARS-CoV-2 is being dubbed as one affecting the elderly or those with a compromised immune system. Surely, these two cohorts make up the bulk of its victims. Yet, simultaneously, it’s being othered as a “Chinese disease,” or, as Donald Trump calls it, “Kung Flu,” which demonizes a nation of people as well as Chinese Americans. It is for this very reason why the WHO named it COVID-19 so that it had no affiliation with a location, group of people or animal to cause stigmatization. The BBC has reported an increase in racist and anti-Asian attacks in the U.S. against Asian Americans since the start of the pandemic with some 1,800 recorded as of late June. A similar characterization was done to Haitians during the AIDS epidemic when the CDC singled out Haitians (the only ethnic group) as being of high risk, because some 20 patients had shown up with symptoms at a hospital in Miami. The warning vilified Haitian Americans for bringing the disease to the U.S. and resulted in some Haitian Americans losing their jobs, housing and admissions to school. The Food and Drug administration subsequently banned Haitians from donating blood. Compelling research in 2016 has since suggested through genetic sequencing that the disease, originating in the Congo, likely entered the U.S. from Haiti, but it was not then known as fact. While the stigmatization of Haitians has largely been forgotten, it persisted with the gay community.
By othering the disease with a certain group of people in either case, it gives the disease a face, right or wrong, that can be misleading or cause harm to those whom it vilifies. If you are young or have no underlying conditions, you can take your chances with COVID-19 because the odds are in your favor, but while this is statistically true, there have been countless reports of otherwise healthy people: young, fit, athletic, and even medical professionals who would be the most keen on the disease that have succumbed. Unlike other diseases, COVID-19 is wily and unpredictable showing a range of symptoms, even none at all in 40% of cases who can still pass on the infection. It’s able to hijack the body’s systems to cause organ failure, even in healthy bodies, and the reasons for why it can do this some amount of the time is still unknown. How many people deemed as having the lowest risk would willingly stand before a loaded shotgun, knowing that some 7.5% of the time they will get a direct and fatal hit? But even though SARS-CoV-2 has a stigma, it doesn’t yet appear to be one that is feared enough. So, people take their chances.
Another factor that minimizes the stigma of COVID-19 and mitigates the public fear is that COVID-19 has so far been a hidden disease. With shelter in place policies and strict CDC guidelines to regulate the health care system, those afflicted with the disease are at home or alone in the hospital where cameras don’t show an unfiltered perspective of the suffering. In the 80s, HIV patients were shown wasting away like living corpses with lesions everywhere, and while there’s some public understanding that COVID-19 is nasty, the public mostly hears second-hand accounts from healthcare workers or survivor stories, as they get applauded leaving the hospital. It makes the disease appear abstract. Juxtaposed with the glorification, maybe even celebratory in its dissonance. The public doesn’t see the patients’ faces or their grim reality of being unconscious on life support. They hardly, if ever, see the body bags or the mass graves that are routinely shown in other countries, all of which would add to a formulation of fear and stigma.
There have been several reports of people either thinking the disease is a hoax, trying to get it deliberately to build herd immunity, and even some young people who’ve been throwing COVID parties in Texas and Alabama to see if they can contract it from a positive person for sport. This raises the specter that there is some faction of people who are unconcerned about the illness and even willing to get it. A recent Gallup poll has estimated as many as 44% of those surveyed said they are not worried about the disease. When examined along party lines 85% of Democrats are at least somewhat worried, 66% of Independents, and only 47% of Republicans. This finding affirms that the public is possibly being influenced by their political leaders and the framing of that perspective in the media they consume. The unfortunate death of Richard Rose, a 37-year old veteran and Trump supporter, from Clinton, Ohio, who called the disease a hoax and fervently objected to wearing a mask for months on Facebook, said in April, “I’ve gotten sick of turning my tv on to political smear ads and shit about COVID. So yesterday I turned my cable box in. I’ve also started snoozing people on here. It’s time to block out negativity.” On July 1st, he posted that he had contracted the virus. He was dead two days later.
A 2019 research paper backed by the National Institutes of Health (NIH) describes health-related stigma as “a personal experience related to a health condition, characterized by the perception of exclusion, rejection, and blame, and contributes to psychological, physical, and social morbidity.” These health conditions may include those that are deemed contagious, incurable, or harmful, as well as from behaviors considered taboo or immoral. The paper goes on to say, “Stigma starts when salient differences between people are recognized, labelled, and connected to stereotypes or social identities. This process leads on to a separation between ‘us’ and ‘them’, resulting in status loss and discrimination.”
This is observed in the treatment of sufferers and survivors of other diseases like Ebola, SARS, or leprosy, for example. The researchers also suggest that stigma can take root and be maintained via “a dynamic process enacted through structures and individuals, mediated by relationships of power and control that are constantly being produced and reproduced.” So, stigma reinforces itself if you let it happen and can be weaponized by the powerful against the powerless.
The above finding may explain why gay men were easy targets in the 80s and perhaps why your beloved grandfather and grandmother, or someone else’s, escape this kind of reproach for now. It also explains why the plight of those gay men weren’t taken seriously. But it exposes an awful truth as well, which is at the root of the differences between the perception of both diseases. Because HIV was a disease thought largely caught through sexual activities, and specifically anal sex between men, or via intravenous drug use, it was considered dirty and got a scarlet letter. To catch SARS-CoV-2 one need only be exposed to someone’s cough, sneeze or breath. Different body parts seem to have different reputations and should be judged differently. It makes it easier to cast blame on a person infected with HIV because they are “responsible,” and “should know better,” or “could have avoided it by protecting themselves,” let alone doing acts many considered morally reprehensible or even disgusting. But everyone sneezes and coughs and people exposed to SARS-CoV-2 or who refuse to wear masks don’t receive the same kind of judgment. This, of course, isn’t helped by what is being ejected daily from the president’s mouth and Twitter feed.
What is remarkable is that the fear and demonization of HIV sufferers still persists today 40 years later, even as HIV has morphed from being a gay man’s disease to one where anyone is susceptible like COVID-19. And yet, HIV is still considered to be a gay man’s disease, because gay men have a higher risk and heterosexuals as a group are largely free from discrimination and, therefore, stigma.
So, there is some duality with health-related stigma. On the one hand, it garners more public, political and scientific attention when it’s present, but on the other hand it’s deleterious to those who are stigmatized. And this is true for those with the virus or those within proximity to the virus like healthcare workers or family members.
Knowing these facts and the history of the stigmatization of HIV and AIDS, it behooves the media and public officials, including the president, to ensure that SARS-CoV-2 doesn’t go down the same path. Sanctioned discrimination and discriminatory policies create a hotbed of issues for those on the receiving end psychologically, in gaining access to services like housing, employment, or even seeking treatment. This was true for Haitians in the 80s, is true for those with HIV/AIDS as well as those suffering from non-pathogenic disorders like substance abuse today. We’ve already seen how SARS-CoV-2 and HIV have impacted marginalized communities. Consider also the historical difference in treatment of the African Americans afflicted by the crack epidemic, who were branded as criminals and outcasts, compared to today’s largely white opioid addicts, who are “suffering from mental health issues.” Perspective and messaging, especially from trusted officials, influence public opinion and outcomes. As the NIH research paper suggests, a stigma will take hold when a group can be labeled and discriminated against, especially if they are stereotyped and powerless.
The Black, brown and LGBTQ communities typically work in jobs that leave them unable to work from home for the most part and therefore expose themselves to COVID-19 more readily. Both communities have poorer health and the least access to healthcare of any other community. The elderly, too, can become perfect victims and scapegoats should the virus persist since they are the most susceptible to this disease from a health perspective. If left unchecked, any unanticipated or unforeseen fallout from this novel virus could land in the laps of all or either three populations, being amongst the most vulnerable or poorest.
While no deep-rooted stigma has yet taken root with COVID-19 to make many consider its victims as deserving or to blame for their condition or mistreatment like various Asian Americans have been, we must avoid a certain complacency and complicity to sacrifice those whose lives we can disregard or whose immune systems we think are just not strong enough. In a fight like this, everyone has to band together, because our lives, collective health and well-being depend on it.![]()